BNA Annual General Meeting 2025
1st April 2025


We have collated a number of resources below that can be used for teaching or to kickstart further research. Each resource has been seperated by topic/subject. If you know of or have created any resources that you believe would be useful in this section please contact: office@bna.org.uk
Contents |
This article addresses the value of diversity in STEM. Highlighting the positive outcomes of diversity such as the production of excellence through diverse working groups, the ability for unrecognised talent to thrive, economic growth and increased global competitiveness within STEM.
 Undergraduate Neuroscience Education, 11(1), A52.
Undergraduate Neuroscience Education, 11(1), A52.The lack of racial and ethnic diversity in STEM fields requires immediate attention. Weekes (2012) argues for immediate action in four specific directions. Weekes states that we need to continue to recruit and incentivize the mentoring of a diverse pool of junior faculty. We need to introduce Under-Represented Minority (URM) students to “science in practice” through our research labs as early as possible and we need to provide the resources to allow URM students to succeed in STEM fields. Lastly, he argues that we need to encourage students of all backgrounds to “reach back” and involve themselves in science within higher education.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3592754/

Oliver Rollins is a sociologist interested in how neuroscience research deals with and is informed by racialisation, racism, and other social processes of inequality. Within this article he discusses how neuroscientists and others working within STEM can engage in antiracist research practices and in turn contribute towards an antiracist (neuro)science.
https://doi.org/10.1038/s41562-021-01075-y

“2020: The year of inclusion, scrapping labels, where previous divisions become archaic and dated”. In this article, Shyamsundar, Asaria and Bajra (2020) highlight the experiences of Black, Asian and Minority Ethnic scientists as they have progressed through the decades. They go on to discuss the possibility of a future without inequality within STEM subjects and industries.
https://portlandpress.com/biochemist/article/42/3/54/225279/BAME-scientists-the-hidden-pioneers
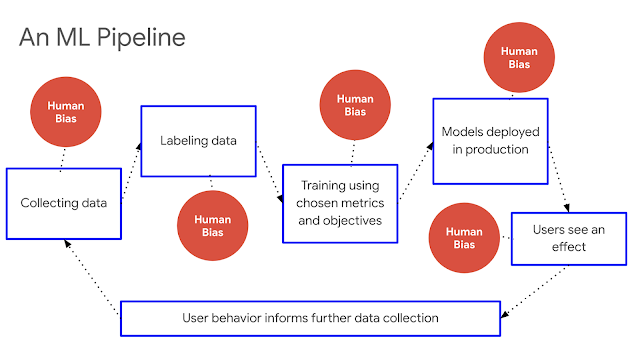 .
.With the integration of AI into various sectors and applications, the issue of bias in AI has rightfully come to the forefront of discussion. Recognizing and addressing bias in generative AI models is crucial to building inclusive technology which ensures diverse perspectives are factored, and that outcomes are both fair and equitable.
https://aifwd.com/field/building-inclusive-ai-strategies-for-training-against-racism/

Antonio et al., (2004) are investigating the effects of racial diversity on complex thinking in small group discussions within college students. They are assessing 357 students across three universities to determine the effect size on complexity. Results showed that racial and opinion minorities were both perceived as contributing to novelty. Generally positive effects on integrative complexity were found when the groups had racial and opinion-minority members and when members reported having racially diverse friends and classmates. The research supports claims about the educational significance of race in higher education, as well as the complexity of the interaction of racial diversity with contextual and individual factors.
https://journals.sagepub.com/doi/abs/10.1111/j.0956-7976.2004.00710.x

Diversity breeds innovation, yet underrepresented groups that diversify organizations have less successful careers within them. Hofstra et al., (2020) found that demographically underrepresented groups innovate at higher rates than majority students. However, their novel contributions are often devalued and discounted. An example would be how novel contributions by racial minorities are taken up by other scholars at lower rates than novel contributions racial majorities. Equally impactful contributions of racial minorities are less likely to result in successful scientific careers than for majority groups. These results suggest there may be unwarranted reproduction in academic careers that discounts diversity’s role in innovation and explains the underrepresentation of some groups in academia.
https://www.pnas.org/content/117/17/9284.short

We introduce a general framework for modelling functionally diverse problem-solving agents. In this framework, problem-solving agents possess representations of problems and algorithms that they use to locate solutions. We use this framework to establish a result relevant to group composition. We find that when selecting a problem-solving team from a diverse population of intelligent agents, a team of randomly selected agents outperforms a team comprised of the best-performing agents. This result relies on the intuition that, as the initial pool of problem solvers becomes large, the best-performing agents necessarily become similar in the space of problem solvers. Their relatively greater ability is more than offset by their lack of problem-solving diversity.

During the Dark Ages the “medical flame” was set alight by the Arabic-Islamic world. The period between the 7th and 13th centuries has been commonly neglected, despite the remarkable developments of biomedical science of the Arabic-Islamic (Falagas et al., 2006). At every stage in Arabic medical history, we can find outstanding people whose greatest contributions and efforts cannot be underestimated. This journal illustrates the advancements in Arabic-Islamic science with some examples of those whose books contributed towards the development of Medieval European neuroscience.
In his Al Hammadi Lecture at the Royal College of Physicians of Edinburgh, John Urquhart, professor of biopharmaceutical sciences at the University of California at San Francisco, contrasted Ibn Sina's Canon of Medicine (c. 1012) with Osler's Principles and Practice of Medicine. Urquhart asked himself which of the two books he would want if he was marooned and in need of a guide for practical medicine. He opted for Ibn Sina's Canon because the book presents an integrated view of surgery and medicine. Ibn Sina tells his readers, for example, how to judge the margin of healthy tissue to remove with an amputation. In contrast, Osler shunned intervention in his Principles and Practice of Medicine. The enduring respect in the 21st century for a book written a millennium earlier is testimony to Ibn Sina's achievement.
https://journals.sagepub.com/doi/full/10.1258/jrsm.2008.08k040
Within a century after the death of Prophet Muhammad (peace be upon him) the Muslims not only conquered new lands, but also became scientific innovators with originality and productivity. By the ninth century, Islamic medical practice had advanced from talisman and theology to hospitals with wards, doctors who had to pass tests, and the use of technical terminology. These medical centres contained libraries, pharmacies, the system of interns, externs, and nurses. There were regulations to maintain quality control on drugs. Pharmacists became licensed professionals and were pledged to follow the physician's prescriptions. Legal measures were taken to prevent doctors from owning or holding stock in a pharmacy. The article explains the extent to which Islamic medicine advanced in the fields of medical education, hospitals, medicine and psychotherapy.
http://al-hakawati.net/Content/uploads/Culture/1293_Islamic_Medicine_Ahead_of_its_Time.pdf
Since the application of technical medicine by the Greeks, modern neurology has been based on a body of knowledge and cultural heritage from ancient times. In this paper Martin-Araguz et al., (2002) review the contribution made by Al Andalus to neuroscience during the Middle Ages and its repercussions on modern neurology. Andalusian doctors made major contributions to the body of knowledge about neuroscience and developed major philosophical concepts of human understanding. Abulcasis (936 1013), the father of modern surgery, developed material and technical designs which are still used in neurosurgery and Averroes suggested the existence of Parkinsons syndrome and attributed photoreceptor properties to the retina.

This review addresses this issue of psychedelics in science and the limitations of white-dominant medical framework directly. Firstly, George et al., (2020) highlight the traditional role of psychedelic plants and summarised the history of psychedelic medicine. They later go on to discuss the historical and sociocultural factors that have contributed to unequal research participation and treatment. They argue that this unequal research participation has limited the opportunities for minorities to contribute towards science. Finally, they provide an agenda for Western medical framework of healing to include a cultural focus and additional considerations for an inclusive approach to treatment development.
https://akjournals.com/view/journals/2054/4/1/article-p4.xml

African American women are disproportionately underrepresented in the domains of science, technology, engineering and mathematics (STEM) in relation to their share of the United States population. Charleston et al., (2014) utilise intersectionality theory as a theoretical foundation to explore the role race and gender play in the STEM pursuits of African American women, offering suggestion of some of the strategies this population uses to accomplish STEM educational goals.

Cantor et al., (2014) argue that the utilisation of intersectionality and diversity in research is invaluable. They suggest that an intersectional approach offers a powerful means of producing new knowledge and the more fully human social and institutional practices that will be essential for improving the quality of life for both majority and minority populations in the twenty-first century.
https://www.proquest.com/docview/1628947079?pq-origsite=gscholar&fromopenview=true

This paper aims to discuss the term intersectional trap. This is defined as the act of saying blanket statements to describe a race or group of individuals without considering variations of experience within the population. This article also provides some suggestions for research focusing on qualitative studies that explore the lived experiences of students as they form their science, technology, engineering and mathematics (STEM) identities. Finally, this article discusses the need for an intersectionality lens when considering how to retain talented female students of colour in university STEM programs.
https://www.emerald.com/insight/content/doi/10.1108/JME-12-2015-0049/full/html

This article draws on critical race theory and the experiences of people from marginalized groups in STEM to support the need for intersectionality in STEM education research. It also offers a critique of apolitical discipline-based STEM education research and integrated STEM education that fails to consider intersectionality. The authors identify ways in which STEM education researchers can facilitate collaboration across education equity communities and conduct research with the power to mitigate oppressive forces in STEM education and in the STEM workforce.
 In this chapter, Ireland et al., (2018) argue that intersectionality is a theoretical and methodological framework by which education researchers can critically examine why and how students in STEM fields who are members of intersecting marginalized groups have distinctive experiences related to their social identities, other psychological processes, and educational outcomes. Additionally, they have found that the current discourse on intersectionality is limited in that it does not attend to key psychological processes associated with identity and the intersectional experience in STEM education. This article highlights the ways that researchers have employed intersectionality to make the experiences of Black women and girls in STEM education more visible, or “unhidden.” https://journals.sagepub.com/doi/abs/10.3102/0091732X18759072casa_token=khw43_U_wEMAAAAA:4wXxXwAEe9A_3gt2tYx9WLxp8-5IexMmyFfSNuNqp-bd88lKmjaEHeVuPPnSMl4PJuwhHQWzikY
In this chapter, Ireland et al., (2018) argue that intersectionality is a theoretical and methodological framework by which education researchers can critically examine why and how students in STEM fields who are members of intersecting marginalized groups have distinctive experiences related to their social identities, other psychological processes, and educational outcomes. Additionally, they have found that the current discourse on intersectionality is limited in that it does not attend to key psychological processes associated with identity and the intersectional experience in STEM education. This article highlights the ways that researchers have employed intersectionality to make the experiences of Black women and girls in STEM education more visible, or “unhidden.” https://journals.sagepub.com/doi/abs/10.3102/0091732X18759072casa_token=khw43_U_wEMAAAAA:4wXxXwAEe9A_3gt2tYx9WLxp8-5IexMmyFfSNuNqp-bd88lKmjaEHeVuPPnSMl4PJuwhHQWzikY

NINDS discusses strategies at multiple systemic levels where opportunities and interventions could be implemented to enhance neuroscience workforce diversity.
https://www.sciencedirect.com/science/article/pii/S0896627320304876

This journal highlights the issue of intersectionality for people within STEM careers. The Campaign for Science and Engineering argues that women, ethnic minorities, and those with disabilities are consistently underrepresented, particularly at senior levels, in STEM. Diversity issues also persist in other sectors; however, this report focuses on improving diversity in STEM due to the existence of STEM-specific barriers and challenges, and the significant benefits that improving diversity in STEM would bring for individuals and for the UK.
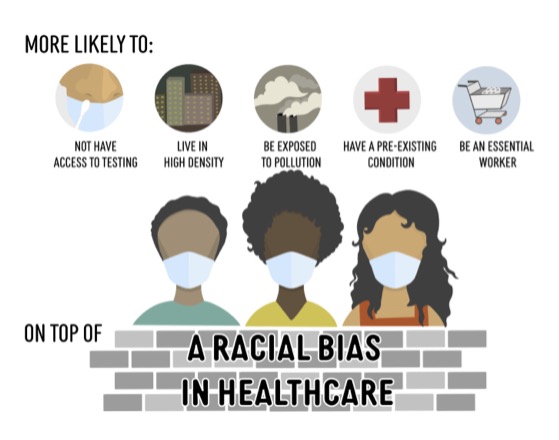
This article argues that structural racism is a fundamental factor of racial and ethnic disparities in health. Razai et al., (2021) argue that structural racism is a cause of ethnic differences in socioeconomic status, adverse health outcomes, and ethnic inequities in health. They state that new government approach on race is divorced from reality and fails to provide any solutions to ethnic disparities in health. They believe it undermines the well-established and evidence-based role of ethnicity on health. Therefore, they suggest that outcomes will lead to a worsening of systemic inequalities, putting more ethnic minority lives at risk.
This literature review aims to identify the barriers and enablers for recruiting people from Black, Asian and Ethnic Minority communities in research. A thematic analysis was applied to 39 papers to identify the key issues for consideration when conducting health related research with Black, Asian and Ethnic Minority communities. A number of key themes were identified as potential barriers these included language use and ability, socio-cultural factors such as issues with someone’s ethnicity, lack of knowledge about research and practical issues such as cost implications of research.
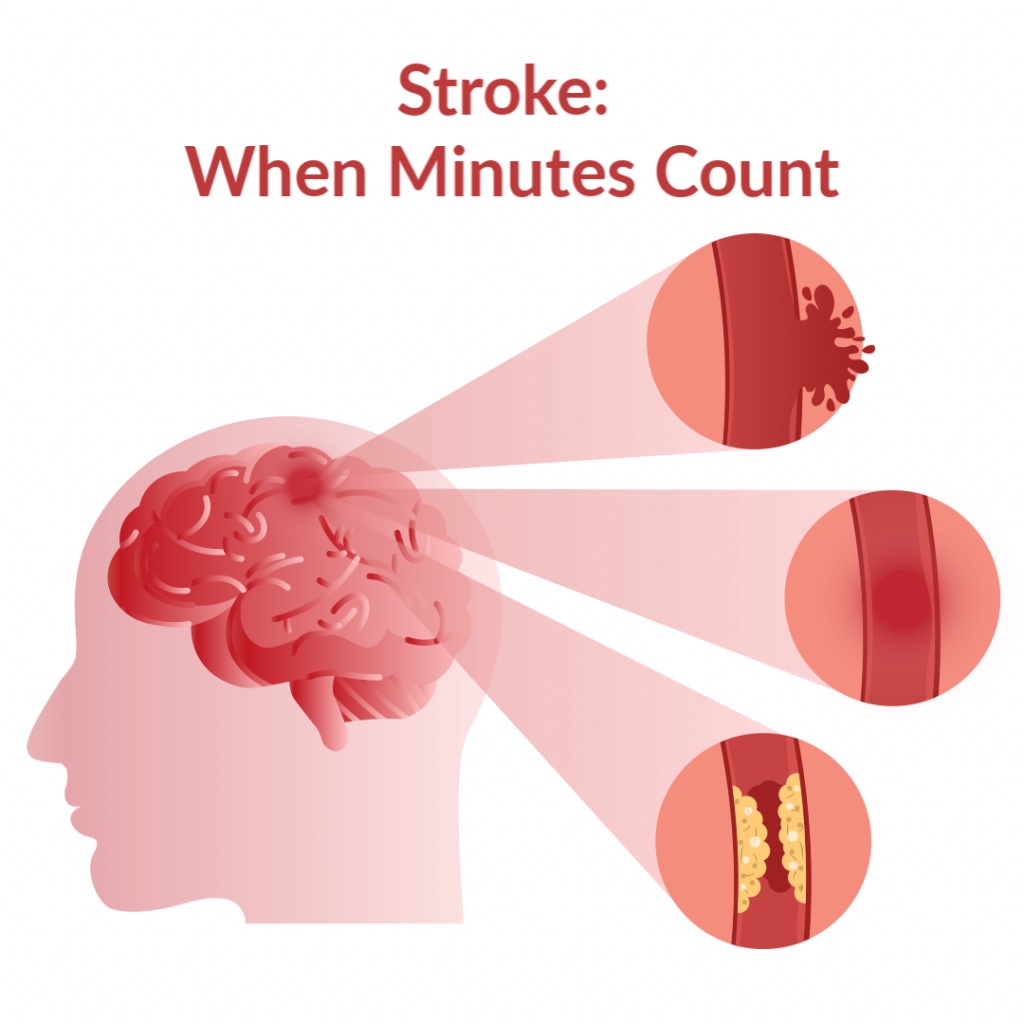
This article highlights the excess stroke mortality rate among African Americans that they argue should be considered a national crisis. Only a portion of this excess stroke mortality among African Americans can be explained by the higher prevalence of hypertension and diabetes in African Americans, and by the lower average socioeconomic status (SES) among African Americans. The majority of the excess burden of stroke mortality is affecting those between the ages 35-64 who are African Americans living in the South-eastern United States. While overall stroke mortality rates have been rapidly declining the magnitude of the relative increased risk of dying from a stroke among African Americans has remained largely unchanged. They argue that efforts to reduce ethnic disparities in stroke mortality have been unsuccessful.
https://europepmc.org/article/med/11763299
 Association. Stroke, 42(7), 2091-2116.
Association. Stroke, 42(7), 2091-2116.The purpose of this article is to describe the effect of race and ethnicity on stroke epidemiology, personal beliefs, access to care, response to treatment, and participation in clinical research. Cruz-Flores et al., (2011) acknowledge that the state of knowledge on the main factors that may explain disparities in stroke care have gaps that need to be filled to guide future research. Acknowledging the presence of disparities and understanding the factors that contribute to them are necessary first steps.
https://www.ahajournals.org/doi/full/10.1161/STR.0b013e3182213e24

Evidence for ethnic disparities in stroke incidence, severity, and mortality has continued to rise over the past few decades. However, for disparities in acute management and rehabilitation remains more ambiguous. The objective of this report is to summarize the current evidence from stroke epidemiology and studies focusing on disparities in stroke care and disability, while also suggesting courses for action. Minority ethnic groups have higher rates or more severe stroke, but variations in prognosis for clinical outcomes other than mortality remain less certain.
https://www.ahajournals.org/doi/abs/10.1161/01.STR.0000153065.39325.fd

Systemic racism is a public health crisis. Systemic racism and racial/ethnic injustice produce racial/ethnic disparities in health care and health. Substantial racial/ethnic disparities in stroke care and health exist and result predominantly from unequal treatment. This report aims to highlight selected mediations to reduce racial/ethnic disparities in stroke prevention and treatment. Levine et al., (2020) review the social determinants of health and the determinants of racial/ethnic disparities in care. This article also summarises selected interventions aimed at reducing stroke risk factors, increasing awareness of stroke symptoms, and improving access to care for stroke because these interventions hold the promise of reducing racial/ethnic disparities in stroke death rates. Finally, Levine et al., (2020) acknowledge the gaps in research and suggest future directions.
https://www.ahajournals.org/doi/abs/10.1161/STROKEAHA.120.030427

Pathak & Sloan (2009) have analysed the 2001–2006 trends in stroke hospitalizations and hospital case-fatality for black, Hispanic, and white adults aged 25–49 years in Florida. They found that age-adjusted stroke hospitalization rates for black Americans were over three times higher than rates for white Americans. The in-hospital fatality rate for all strokes was highest among black Americans at 10% compared with 9% of white Americans and Hispanic Americans at 8.2%. Conclusively, Pathak and Sloan (2020) discovered a strong and persistent black-white disparity in stroke hospitalization rates for young adults.
https://www.karger.com/Article/Abstract/208795
Gutierrez et al., (2014) evaluate the prevalence that vascular risk factors account for differences observed in stroke subtypes by race/ethnicity. Patients with acute stroke were prospectively enrolled in the Miami Stroke Registry. Patients’ demographic, clinical and radiological characteristics were systematically collected. The Five subtypes of Ischemic stroke were ascertained using the TOAST criteria. The sample was divided into Non-Hispanic Whites (NHW), Hispanics, African Americans (AA), and Non-Hispanic Black Caribbean (NHBC). Their results suggest that the vascular risk factors prevalence among different racial and ethnic groups partially explains disparities found in the prevalence of some stroke subtypes.

This journal reviews the evidence for mental health and mental health care disparities, comparing them to patterns in health. McGuire & Miranda (2008) highlight strategies for addressing disparities in health care, such as improving access to quality of care and should also work to eliminate mental health care disparities. In addition, they suggest that a diverse mental health workforce, as well as provider and patient education, are important in eliminating mental health care disparities.
https://www.healthaffairs.org/doi/abs/10.1377/hlthaff.27.2.393
Primm et al., (2010) have argued that racial/ethnic minority populations are underserved in the American mental health care system. They put an emphasis on the disparity in treatment between whites and African Americans that has increased substantially since the 1990s. Primm et al., (2010) present a model that illustrates how social determinants of health, interventions, and outcomes interact to affect mental health and mental illness. Primm et al., (2010) suggest that public health approaches to these concerns need enhanced surveillance and new public-policies to improve standards and reduce disparities.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2811515/

Blanco et al., (2007) compare trends in office-based treatment of mental disorders between Hispanics and non-Hispanics. From 1993 to 2002, there was an increase in mental health care disparities between Hispanics and non-Hispanics treated by office-based physicians. They highlight the importance of the mental health care for Hispanics as a public health priority, with clear opportunities and challenges for health care policymakers and practitioners.
https://www.jstor.org/stable/40221575?seq=1#metadata_info_tab_contents

Marrast et al., (2016) examine racial and ethnic disparities in children’s and young adults’ receipt of mental health and substance abuse care using nationally representative data from the 2006–2012 Medical Expenditure Panel Surveys. Disparities were generally larger for young adults than for children. Black and white children had similar psychiatric inpatient and emergency department utilization rates, while Hispanic children had lower hospitalization rates. Marrast et al., (2016) concluded that psychiatric and behavioural problems among minority youth often result in school punishment or incarceration, but rarely mental health care.
https://journals.sagepub.com/doi/abs/10.1177/0020731416662736
This study compared trends in racial-ethnic disparities in mental health care access among whites, blacks, Hispanics, and Asians by using the Institute of Medicine definition of disparities as all differences except those due to clinical appropriateness, clinical need, and patient preferences. No reductions in racial-ethnic disparities in access to mental healthcare were identified between 2004 and 2012. For blacks and Hispanics, disparities were exacerbated over this period. Clinical interventions that improve identification of symptoms of mental illness, expansion of health insurance, and other policy interventions that remove financial barriers to access may help to reduce these disparities.
https://ps.psychiatryonline.org/doi/abs/10.1176/appi.ps.201500453
This study examined racial and ethnic differences in treatment outcomes among participants in a randomized controlled trial of an intervention for first-episode psychosis called NAVIGATE. In usual community care, non-Hispanic blacks scored higher on measures of psychiatric symptoms and were less likely to receive important services, compared with non-Hispanic whites. In NAVIGATE, racial and ethnic differences in psychiatric symptoms were not evident, although non-Hispanic blacks were less likely than non-Hispanic whites to receive family psychoeducation.
https://ps.psychiatryonline.org/doi/abs/10.1176/appi.ps.201800067
Szaflarski et al., (2006) have examined the understanding of the minority disadvantage in the clinical management of epilepsy. Research concerning racial/ethnic differences in epilepsy treatment is scarce and limited by methodology, while also suggesting underutilization of state-of-the-art therapies by minorities. They proposed a framework to identify the array of disparities, points of intervention, and interventions.
https://www.sciencedirect.com/science/article/pii/S1525505006002058

The International League Against Epilepsy undertook a systematic review of the evidence on disparities in epilepsy with a focus on North American data (Canada, United States, and the English-speaking Caribbean). They have identified access to and outcomes following medical and surgical treatment, disability, incidence and prevalence, and knowledge and attitudes. An exhaustive search (1965–2007) was done, including: (1) disparities by socioeconomic status (SES), race/ethnicity, age, or education of subgroups of the epilepsy population; or (2) disparities between people with epilepsy (PWE) and healthy people or with other chronic illnesses.
https://onlinelibrary.wiley.com/doi/full/10.1111/j.1528-1167.2009.02282.x

This study aimed to identify whether race/ethnicity and limited English proficiency impact the likelihood of pursuing surgical treatment for medically refractory epilepsy. Demographic and clinical factors potentially associated with surgical utilization, including self-reported race/ethnicity and preferred language, were gathered from the medical record. Betjemann et al., (2013) found that race and limited English proficiency contribute to disparities in the surgical management of medically refractory epilepsy, especially among Asian/Pacific Islanders and African Americans.
https://www.sciencedirect.com/science/article/pii/S1525505013002989

The purpose of this study was to compare the use of surgical treatment for epilepsy among different ethnic and racial groups with surgically remediable temporal lobe epilepsy (TLE). Of 432 patients diagnosed with TLE, 130 had evidence of mesial temporal sclerosis on MRI studies. Seventy patients underwent surgery; African Americans were less likely than non-Hispanic whites to undergo surgical treatment. African Americans had a 60% less chance to receive surgery than non-Hispanic whites. They concluded that there are disparities in the use of surgical treatment for temporal lobe epilepsy and race appears to be an influential factor related to such disparities.
Zuckerman et al., (2008) investigated differences in anti-dementia medication use between non-Hispanic White and minority community-dwelling Medicare beneficiaries with dementia. Presenting numerous studies, they have documented disparities in health care utilization between non-Hispanic White and minority elders.
https://academic.oup.com/psychsocgerontology/article/63/5/S328/592324?login=true
The purpose of this study was to evaluate the utilization of anti-hypertensive and dementia drugs and adherence in a national cohort of veterans aged 65 years or older with a diagnosis of both hypertension and dementia across different racial/ethnic groups. Poon et al., (2009) found that racial/ethnic differences exist in anti-hypertensive and dementia medication use in a cohort of older adults with hypertension and dementia. They believe that healthcare providers should make special efforts to improve medication adherence among minorities.
https://journals.sagepub.com/doi/abs/10.1345/aph.1l368
The aim of this study was to analyse national data on variations in the uptake of anti-dementia medication between people with young-onset dementia (YOD) and late-onset dementia (LOD). Findings highlight the impact that social factors and ethnic disparities have on current usage of anti-dementia medication and the need for more resources to enable equitable use of anti-dementia medication.
The aim of this study was to conduct a narrative review of the literature, demonstrating how racial and ethnic disparities manifest across the full spectrum of the traumatic brain injury (TBI) experienced in civilian populations. They argued that understanding racial and ethnic disparities is a first step in ensuring equitable care for all individuals with TBI, including raising awareness among clinicians and guiding the development of tailored interventions for racial and ethnic minority populations.
https://link.springer.com/article/10.1007/s40615-021-01017-4

Sleep may play an important role in health disparities. The main purpose of this review is to examine the potential ramifications of inadequate sleep in a multicultural context; to identify cultural variations between patient and provider in the delivery of sleep care, borrowing from the medical and psychosocial literature; and propose potential strategies to address sleep disparities. They sum up this review with a possible agenda for the future of sleep health.
https://www.sleephealthjournal.org/article/S2352-7218(14)00009-6/abstract
 Jackson, C. L., Powell-Wiley, T. M., Gaston, S. A., Andrews, M. R., Tamura, K., & Ramos, A. (2020). Racial/ethnic disparities in sleep health and potential interventions among women in the United States. Journal of Women's Health, 29(3), 435-442.
Jackson, C. L., Powell-Wiley, T. M., Gaston, S. A., Andrews, M. R., Tamura, K., & Ramos, A. (2020). Racial/ethnic disparities in sleep health and potential interventions among women in the United States. Journal of Women's Health, 29(3), 435-442. In this review Jackson et al., (2020) describe racial/ethnic sleep disparities and subsequent implications for health from epidemiological and clinical studies. Focussing on factors of intersectionality for female racial minorities.
https://www.liebertpub.com/doi/abs/10.1089/jwh.2020.8329

Ahn et al., (2021) conducted a review of studies on sleep disparities by race/ethnicity to summarize characteristics of existing studies and identify evidence gaps. One hundred sixteen studies were included in this review. Most studies focused on disparities between Whites and Blacks. Disproportionately fewer studies examined disparities for Hispanic, Asian, and other racial/ethnic groups. Self-reported sleep was most frequently used. This review identified significant evidence gaps in racial/ethnic disparities research on sleep. Ahn et al., (2021) results suggest a need for more studies examining diverse sleep features using standardized and robust measuring methods for more valid comparisons of sleep health in diverse race/ethnicity groups.
https://www.sciencedirect.com/science/article/pii/S138994572100126X



